National Minority Health Month: Be the Source for Better Health
April marks an important observance in the healthcare calendar: National Minority Health Month. This month is dedicated to ...



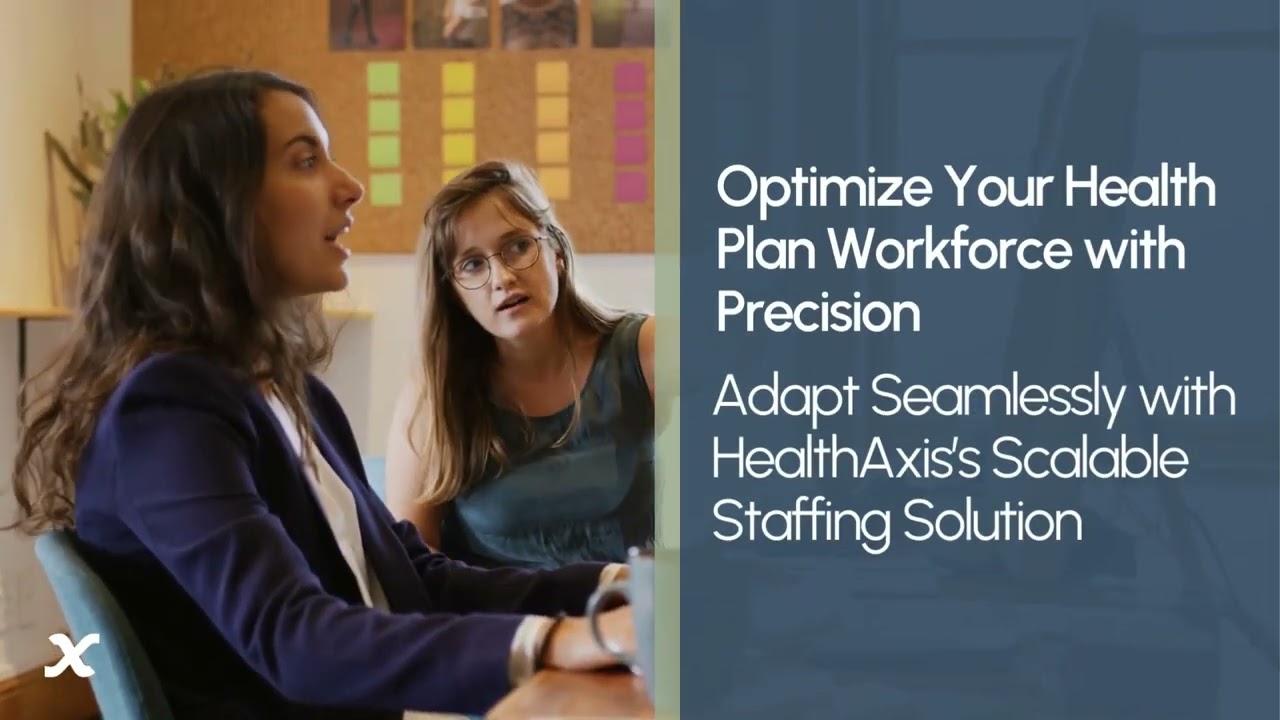
Technology and expertise should not be obstacles but accelerators for your business success. You need solutions that adapt to your unique challenges and scale with your growth.
HealthAxis meets these demands with a suite of services, including our proprietary CAPS technology, BPaaS, BPO, staff augmentation, and consulting. Designed for efficiency and effectiveness, our solutions simplify health plan management, allowing you to concentrate on supporting your members’ healthcare needs.
Our expertise in tailoring services and technologies ensures:






Adapt and grow with our scalable technology & services, designed to evolve seamlessly with your business needs.

Benefit from a holistic approach that ensures seamless coordination across all aspects of your health plan management.

Depend on our comprehensive expertise to guide you through industry complexities, delivering accuracy, compliance, and innovation.

Achieve greater operational flexibility and cost efficiency with our combined services, designed to streamline your processes and support your strategic goals.
Feeling overwhelmed by the demands of your healthcare payer operations? We understand the challenges of staying ahead in a rapidly evolving industry. At HealthAxis, we recognize the stress of managing fluctuating workloads, meeting compliance standards, and sustaining quality member services.
With HealthAxis’s staff augmentation services, you’re not just filling positions; you’re enhancing your team’s capabilities. Our solution offers access to over 130 operational roles, each designed to boost efficiency and effectiveness in your organization.

Solutions

Empowering
Health Plan
Excellence

HealthAxis's client-focused and flexible software and services offerings have created strong relationships with our payer partners. Our use cases are a testament to our commitment to ensuring our client's success.

Stay up to date with the latest healthcare trends and grow your business.

The HealthAxis platform is a user-friendly system that allows for a smooth communication between each application. This allows for multiple departments to handle member customer service in an efficient manner.

We'll discuss challenges with your current system, the services you need and your timeline.
Our team will demonstrate how you can automate tasks and integrate with existing programs.
With your dedicated customer service team, the process is seamless.
With more than 55 years in the industry, we know what works.